Fortunately, things have been much easier with my reversal surgery than my prior surgery, back in January. With my reversal, I was discharged from the hospital two days after the surgery took place. I’m back at work, as of yesterday. My energy levels are good; there were just a few days of fatigue. And my pain at the surgical site has improved; I was able to manage it with just Tylenol after I was discharged, and I haven’t had any Tylenol since yesterday morning.
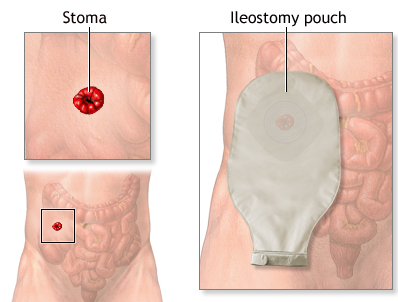
An hour or so before the reversal surgery took place, back on Apr 18, a resident physician (who worked with my surgeon on the procedure), spoke with me briefly about what to expect with the surgery. “Did you give it a name?” she asked. After a few moments of confusion, I realized she was talking about my stoma. I told her no, I never named it (although I did observe this to be a thing that other folks do, noted in the ostomy subreddit and other places). She seemed to be ready to comfort me with any grief I had about the loss of the stoma through reversal surgery. Nope … I felt no sadness about the end of that phase. Yes, it was a pretty enlightening experience, having the ileostomy, but I am certainly ok to move on.
On the morning of my discharge from the hospital, that same resident came by and helped change my dressing over the wound site. The wound was “packed” (gauze was coiled inside the hole in my stomach) and I watched with somewhat horrified fascination as she pulled out that blood-soaked gauze, and applied new dressing. I’ve been doing this same routine on my own, every day since, along with a thorough cleaning of the area via a shower. The hole is already closing up — pretty fascinating to track its progress every day. When I first got out of the hospital, it looked like this surreal second belly button — not too far away from my actual belly button — and a bit wider. Just to clarify, this hole did not go all the way into my innards; the resident explained that it stopped at the layer of my abdominal fascia.
Other than those daily cleanings and dressing changes, the main challenge post-reversal has really been adjusting to having a functioning colon again — with a rectum that is now considerably smaller. I have read several stories of folks dealing with LARS after their reversal and I was prepared for something similar, myself. But things seem to be largely ok with me in the bathroom area, after an initial period of constipation (which I was able to address via Miralax). Bowel movements are certainly more frequent, with associated urgency, but I’m already seeing improvement with this as well, day after day.
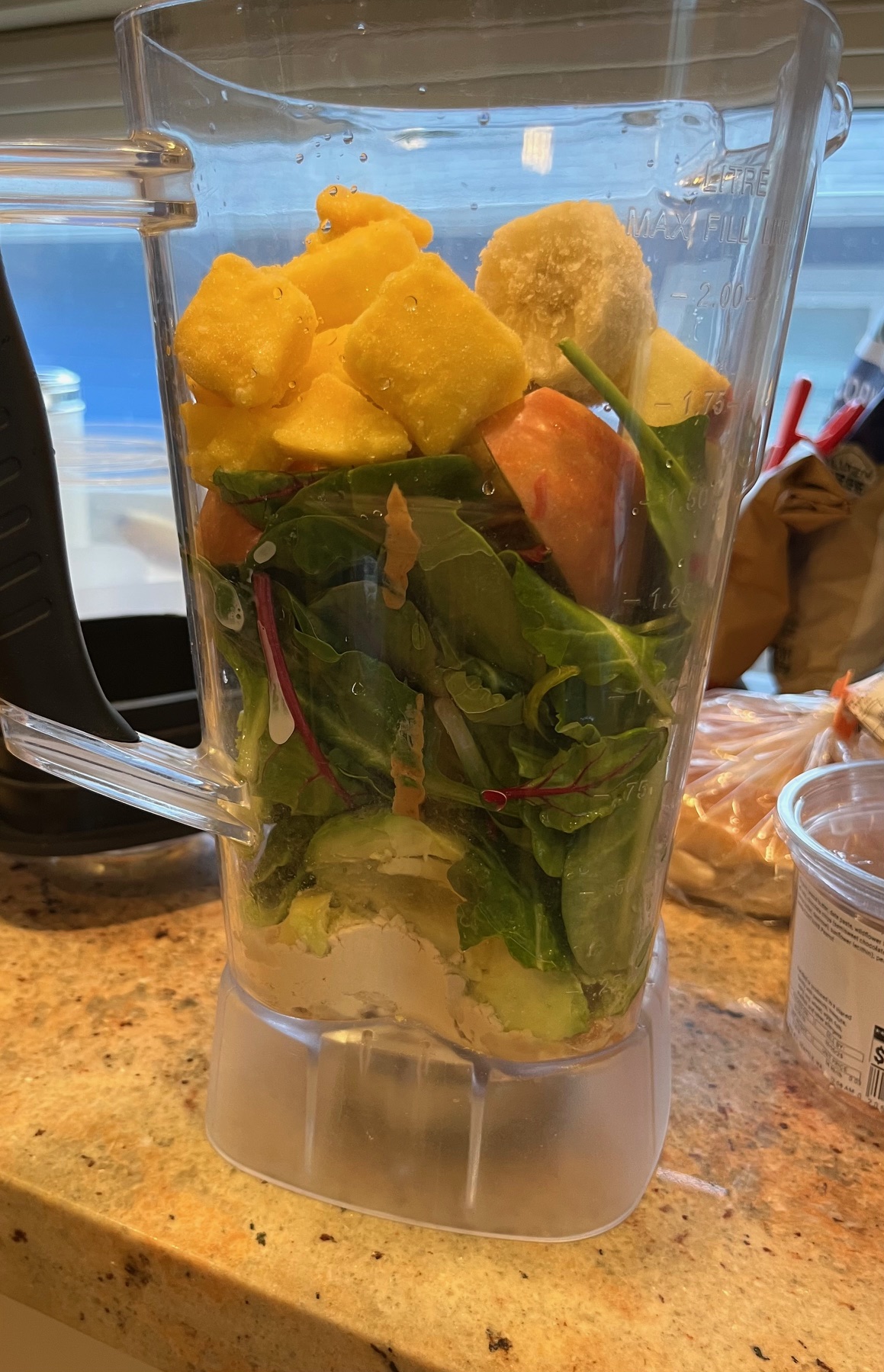
I continue to derive tons of helpful information from the Colontown family of online forums; yes they have one specifically dedicated to all things reversal (“Reversal Roundabout.”) From there, I learned that a first order of business for many folks after their reversal is to restore their gut’s bacteria through probiotics. The challenge is that with a reversal surgery –as with the LAR surgery before it — you get stuck on a restrictive low-fiber diet, which excludes most of the effective dietary sources of probiotics. So what a lot of folks do, I learned, is drink kombucha, at least up until their dietary guidelines loosen up again. I had never actually tried kombucha before, but decided to give it a shot, starting around a week ago, and I quickly realized I love it! Tasty and refreshing!
A week from now, I have CT scans at Fred Hutch; assuming all is clear from those, I’ll finally be able to start saying I’m NED. Of course, you never know what the scans may reveal. I’ve been tracking a variety of stories in Colontown, and of course not everything is positive. Someone with a Stage 3 diagnosis who started chemo on the exact same day I did, last year, just got news that her cancer is metastasizing and she’s now stage 4. I’ve also read recent posts of stage 4 patients passing away. These are notably poignant when it’s the patient themselves sharing the news of their upcoming demise. That said, I do not have “scanxiety;” instead I’m aware of the spectrum of possibilities that may come out of any CT scan, and will take things one step at a time.