I am really loving being a part of my local CRC community; we’ve got an active text thread today, sharing photos of ourselves in blue. And we are all gearing up for the M’s game on March 30. These tickets are selling fast, but there are still some available, here: Strike Out Colorectal Cancer Day
I cannot believe it’s already March — this year is flying by. March is a big month for the colorectal cancer community. We’re dressing in blue on March 7, and our local PNW group is partnering with the Mariners to promote Strike Out Colorectal Cancer Day (Sunday, March 30th).
Meanwhile, I’m happy to report that my “dietary scope” is expanding. This past Friday, I met with an ostomy nurse at Fred Hutch, and she said at this point (2 months post-surgery) it’s fine to start experimenting more with food. So, I’ve taken some baby steps this weekend; I had an impossible burger and some fries at Red Mill with my kiddo Friday evening, and last night I had some split pea soup that was definitely chunky (carrots, celery etc). I seem to be doing ok thus far, so that’s encouraging.
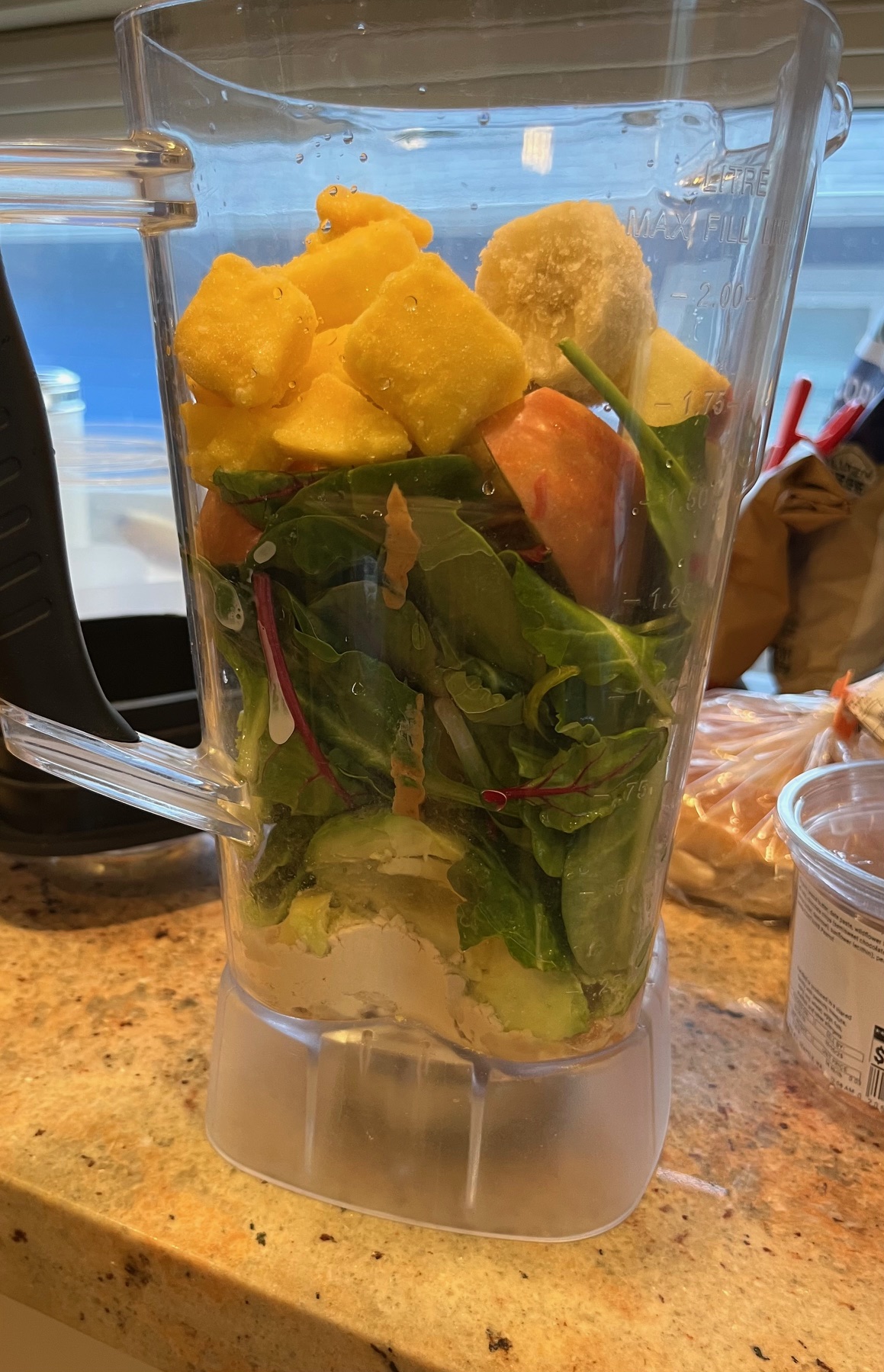
Smoothies continue to be the cornerstone of my daily diet — here’s what went into my smoothie yesterday: generous amount of baby greens (from Trader Joes), frozen banana, frozen mango, apple, avocado, tree nuts (I’ve been alternating between walnuts, cashews, brazil nuts), peanut butter, and pea protein powder. I start off the day with these, and then continue to consume it periodically throughout the day.
Over the past month, I’ve enjoying working with the planning committee for this year’s Seattle Walk to End Colon Cancer. Although the walk will be happening in October, we’re already actively preparing for it. As part of these efforts, I was interviewed in a radio spot that aired this morning on Northwest News Radio.
I’ll be there at the game with other members of the planning committee, helping pass out materials at the booth. Hope to see others there! Buy your tickets before Mar 28.
Over the past week, I’ve been incorporating more and more healthy food into my diet — all via the magic of a blender. My morning smoothies now include apple (peeled), baby greens (kale, chard, spinach), and nuts (walnuts, cashews) in addition to things I’d been including already — protein powder, avocado, bananas. For non-breakfast eats, I’ve been blending up soups with lentils, beans, broccoli, and other vegetables.
Now granted, there has been more than once when I’ve looked at my blended concoctions and note the uncanny resemblance to baby food. I’m basically making a version of baby food for myself, every day. So be it! Blended or no, the fresh greens and nuts are powerful nutrient sources, and I feel much better better after consuming these things. In terms of overall energy level and physical vitality, it’s like a switch from black & white TV, to color TV.
My cousin Kelly will be starting chemo soon, and we’re meeting up this evening so I can bestow upon her the icing kit that I used with many of my own chemo infusions, last year. We discussed meeting up for dinner, and I realized I had a conundrum: is there a local restaurant I can actually eat at, given my current restrictive diet? My go-to is always Asian food (Thai, Japanese), but I can’t eat vegetables, or peanuts, or virtually anything else that is healthy …
After puzzling over this quite a bit, exploring (and then striking out) many options, I sent a message to my care team at Fred Hutch, asking if they had any advice on this. I was happy to hear that they are ok with me beginning to expand my diet, at this point. They explained:
First, you can now advance your diet to include more fiber slowly as tolerated over the course of a couple weeks. The goal here is to introduce fiber one food at a time, chewing well.
Second, you can think about the shape/size of the food to assess the blockage risk. If it is a large chunk, it should be well cooked and/or well chewed.
Third, focusing on soluble fiber first is best as soluble fiber dissolves in water and doesn’t cause bulk, but you can start introducing all kinds of fiber one at a time.
Cool! I am happy about this. Still, however, I wasn’t sure about a restaurant. I was considering Indian food, maybe somewhere where I can get dal or something like that, but it seems like my initial experiment with new dietary options should be at home. Kelly and I have solved this issue by settling on meeting up a dessert place. That’s easier for me — it’s strange but true: less healthy, more processed foods = easier to do with an ileostomy.
But hey, I am very, very ready to move back towards a healthy diet. I mean look what I was doing, back on the morning of my first chemo infusion last summer — an insanely healthy smoothie with chard, kale, various berries .. gotta get back on that train, as this is a key part of the lifestyle to keep my cancer-free, moving forward. So my first venture into healthier eating involves a lentil soup, that I made last night. It includes:
Important to note, after cooking up this soup, I thoroughly pureed it in the blender, to reduce risk of any issues from the lentils. Had this for lunch today (combined with some white rice), and it’s tasty!
I’m realizing a blender is like your best friend, if you’re looking to eat healthy with an ileostomy. Next, I’m planning on starting to incorporate some greens (baby kale) into my smoothies and see how that goes.
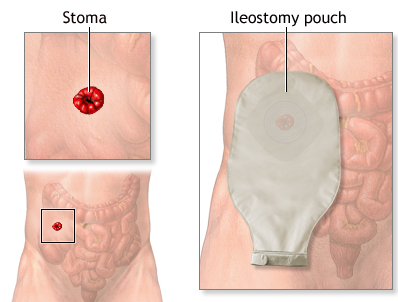
I am currently an ostomate: someone who has an ostomy. My particular type of ostomy is an ileostomy: in the surgery that occurred exactly one month ago today, part of my small intestine, aka ileum, was brought outside (near my belly button), forming an opening called a stoma. Since most of my rectum had to be removed, to rid me of cancer, I now rely on the stoma to excrete my solid waste (which actually isn’t totally solid yet, when it’s in the small intestine). So, I need to always have an ostomy pouch to collect all the “output,” as it’s referred to. I’m going to refrain from posting photos of my stoma and pouch here — I still have several residual scars from the surgery and it just doesn’t look pretty. Instead, here are some generic images.
The stoma is a trip. I’ll always remember the first time I saw it, while I was in the hospital, and a stoma nurse assisted with my first “bag change” (every 3 days, the ileostomy pouch is removed, discarded, and replaced with a new one). It’s like this little pink alien being down there, moving around in its mysterious dance of peristalsis.
Emptying the bag isn’t too bad; you just definitely don’t want it to get too full, or the adhesive seal will start to come undone, which then leads to a messy situation. That happened to me just one time, early on, in the hospital, and I learned my lesson from that. Also, I’m finding you need to embrace loose, high-waisted pants with an ostomy bag. I’m still actually figuring out the clothes thing — I just ordered some special ostomy underwear from Ostomysecrets® (yeah … I know). I’m curious to see if that helps make things more comfortable.
The bag change, which occurs every three days, is a fairly complex procedure. I found early on that you need to do it first thing in the morning, when nothing is coming out of the stoma. You do NOT want any output coming out of the stoma, as you’re doing the bag change. The cute little stoma dance turns into a nightmarish volcanic spectacle … enough said. After removing the old bag, you need to carefully clean all the skin around the stoma. An important step is thoroughly removing the adhesive residue — you do this with a special adhesive remover product.
There are, by the way, all manner of products for ostomy patients. I’ve gotten multiple calls from a popular ostomy product manufacturer; they sent me a gift box of samples and everything. Makes sense — if someone is an ostomate for life, there’s quite a compelling customer lifetime value to capture. Now, the plan is that for me particularly, there isn’t an entire lifetime of revenue that ostomy manufacturers will extract from me, but just a mere three-four months. At that time, the ostomy is supposed to be reversed (scheduling and details still tbd).
Few more notes about the bag change process — after you thoroughly clean the skin, you may need to apply ostomy powder (like diaper powder) on the skin if it’s irritated at all. And then a special product on top of that. And then, you measure the stoma, and you carefully cut out a ring in the adhesive of the new pouch — it needs to be just the right size. This requires special curved precision scissors. And then, you fit the new pouch onto that. There is this additional “caulking” material you can apply, to really get it to adhere .. I generally use that, as well. The whole process takes me around 30 – 40 minutes, including prep.
The real challenge for me is the diet; I need to follow a very restrictive low-fiber diet. It’s unfortunately not a very healthy diet. No fresh vegetables are allowed, at all. Very few fresh fruits are allowed, with the exception of bananas. Anything with seeds (e.g. berries) or peels (tomatoes) are a definite no-no. So I end up eating almost the same thing every day: bagels with creamy peanut butter, bananas, non-dairy yogurt (vanilla only), oatmeal, avocados. It’s this sad irony that I am not able to eat most of the highly-touted cancer-fighting foods right now, like blueberries, walnuts, etc. The dietary restrictions are my least favorite part of the ileostomy experience, but I get the reasoning behind them: you need to avoid anything that might cause a stoma blockage.
Alright, well maybe you’ve learned a thing or two about ileostomies from this post! Feel free to ask me questions if you’re curious about any of this stuff.
Yesterday I met with various members of my care team at Fred Hutch, where I learned a key piece of good news: pathology results from my surgery have been analyzed, concluding that the margins are clean.
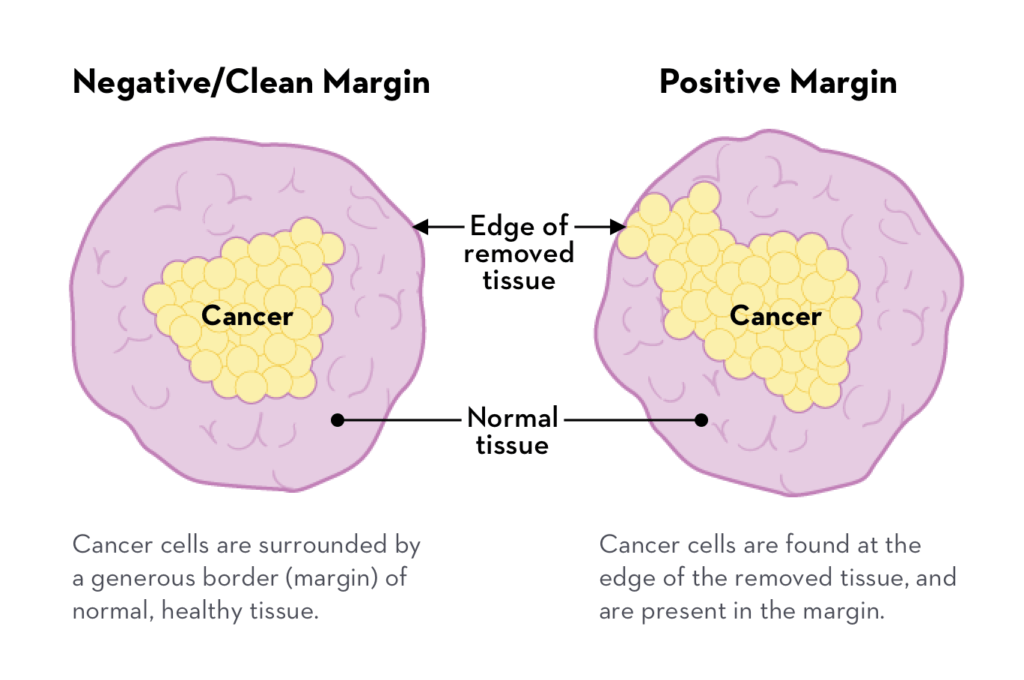
What does this mean? I’ll do my best to explain it, here, as I had no previous familiarity with this terminology. Basically, with a surgery that removes a cancerous tumor, the surgeon cuts out extra tissue that surrounds the tumor. The goal here is to ensure that there are clean margins fully surrounding the excised tumor. I found an image online that breaks this down. A positive (“unclean”) margin is bad news, which apparently can necessitate a followup surgery to cut more out.
Clean margins = surgery success: the cancerous tissue is considered fully removed. But, I asked yesterday, is this equivalent to NED (No Evidence of Disease)? No, they told me. They wouldn’t be able to declare me NED until my next set of scans (not sure, yet, when these will be).
I’m eager to confirm that NED date, honestly because in the colorectal cancer survivor community, everybody celebrates their NED anniversary. Certainly, in years hence, I want to be able to proclaim my NED anniversary as well!
But for the time being, I’ll gladly celebrate all of the information I do have. My last set of scans occurred just a few months ago, in late November. And according to those scans, there wasn’t cancer anywhere in my body, except for the tumor itself — which is now gone. At this time, there is no need for me to do any additional treatment. The big remaining step for me is the ileostomy reversal surgery, which is yet to be scheduled, but may potentially occur sometime in April. I learned yesterday that two diagnostic steps must occur before that surgery: a barium enema (yikes, doesn’t sound fun), and a sigmoidoscopy. They are working on getting those scheduled.
Was my surgery recovery process difficult? Yes, it had its challenges — especially in the first 2 1/2 weeks of recovery time.
Was chemo hard? Definitely.
Did I complain a lot throughout these treatment phases? Yep, just browse through past entries in this blog…
And was it all worth it? Absolutely. This is a no-brainer! These have all been critical steps in ensuring my lifespan is extended. I feel grateful to have had the opportunity to fully focus on the “three act play” of cancer treatment over the past nine months (Radiation, Chemo, Surgery), and am looking forward to shifting my focus to living a normal life, later this year.
Plenty more to share in this blog, though. I haven’t said much yet about life with an ostomy, and associated diet. Also, I’m honored to now be part of the planning committee for the Seattle Walk to end Colon Cancer — I’ll certainly have more to say on that topic in future posts. 🙂
Well, all of those countless hours spent on diligently cleaning my catheter drainage bags were for nought: I got a UTI earlier this week. After a few days of misery in the bladder area, I went to Urgent Care, where the UTI was confirmed via urine sample. Fortunately, I got started on antibiotics right away, and I’m feeling much better.
And in general, I’m doing better every day. Energy level, appetite, and my overall outlook are improving. I’ve started to “lightly interact” with work (checking email, Slack messages, etc) and I’m honestly looking forward to returning full-time on Feb 3.
In other news. my cousin Kelly was diagnosed with colorectal cancer last month. Her diagnosis is eerily similar to mine, but less advanced (lymph nodes not affected). We’ve been chatting, and I’ve been sharing with her what I’ve learned from the past year.
She just shared the news about her diagnosis in a Facebook post, and her story really underscores the importance of screening for colorectal issues. Unlike me, Kelly didn’t have any symptoms. She got a positive result from a LetsGetChecked mall-in test (which led to colonoscopy and diagnosis). While such mail-in tests do not have the same level of granular accuracy as colonoscopies, they are certainly better than doing nothing. I’m so glad that Kelly was proactive, and able to get screened through that method. I’ll be cheering Kelly on, and offering guidance, as she starts her treatment process in the near future.
My lesson over the last few days: post-surgery fatigue can be pretty intense! And for me, it’s notably different from the fatigue that I had with chemo.
Everyone’s experience with cancer treatment varies, but for me, chemo fatigue was mental: my brain was mush and I don’t generally remember those periods. Post-surgery fatigue, by contrast, is totally physical. My mind is ready to go, but my body says: not so fast.
Yesterday, for example, was a very fatigue-y day, with four naps. These were not “fun naps” involving reading or something. No, these were full-on sleep. My big task for yesterday (interrupted by a nap, and a meal, and a period of staring out the window) was changing out all the trash bags in the house, and bringing the trash / compost / recycling outside.
The day before, I possibly pushed myself too much — I took our dog out for a walk around the neighborhood. I was completely exhausted at the end of that, and maybe (?) still recovering the next day. Or, maybe recovery from surgery isn’t always a neatly predictable thing.
Last week, I actually made up a dinner of pancakes and eggs (trust me, things were a lot harder last week … so this was an accomplishment):
I hit a wall, big time, at the end of that — actually I remember I started to fade before I had made all the pancakes; my sister Katy told me hey .. why don’t you take a break there .. but no! I stubbornly insisted on finishing up all the batter, and then collapsed into the recliner, totally spent.
Today was a pretty good day. I am listening closely to my body. I had enough energy to go out for a 15-minute walk –
That was good for the day, and the rest of my time I’ve spent active inside on various tasks. And one big afternoon nap.
Hey everyone, I want to profusely thank my sis Katy for helping with blog posts over these past few weeks. She also helped in countless ways around our house, and with our kiddo, as I have recovered from surgery. Katy headed back home to Eugene yesterday, and I’ll resume writing the posts in this blog.
As mentioned previously, my bladder was nicked during the surgery, resulting in me wearing a catheter for two weeks. Those two weeks are indeed over (thank goodness) — the catheter came out yesterday. I am now basically re-learning how to pee, which is a painful, trial-and-error process. I was hoping to write a celebratory post today about being catheter-free, but it seems I’m not quite out of the woods yet.
Candidly, I’ve struggled with a lot of anger about this whole bladder “nick” and all the misery it’s caused me. Let me just vent a bit. Sometimes we cancer patients just need to vent — here we go:
I had no idea what the #$%& I was doing: As an ostomy patient, I received very detailed (honestly fantastic) instructions and guidance from wonderful ostomy nurses, really focused on day-to-day management of emptying and changing ostomy bags. But there wasn’t anything comparable on life with a catheter, except a video that said I need to clean the drainage bag with bleach every day.
The bleach cleanings: So I think these instructions were maybe(?) excessive, but I was terrified of getting a UTI, so I diligently followed them: any time I changed the catheter drainage bag (twice a day: once in the evening, and once in the morning), I thoroughly cleaned the drainage bag with soap and water, and then let it soak in a diluted bleach solution. This involved using a large syringe to pump the drainage bag full of the bleach solution.
Very limited mobility with the “night bag”: I had a large drainage bag for sleeping, with a hook — if I needed to move around, I carried it by the hook (or tried a few different methods to tote it). The problem was that this bag had large, rather inflexible tubing and I had to move very slowly, very gingerly lest I bump the tubing in just the wrong way: voila, a painful tugging feeling…
Mobility challenges with the “leg bag”: For daytime use, I had a smaller drainage bag that attached to my leg via (uncomfortable) velcro straps. Admittedly, it was easier to walk around with this — kind of. The hospital sent me home with a fabric / velcro strap to secure this to my leg, but that quickly got stretched out, which meant it kept slipping down my leg. Which resulted in that painful tugging feeling..
Lots of time experimenting with hacks: As I was flying blind, I ended up googling alternative catheter securement devices, and bought a few options on amazon — these were adhesive, so I spent a lot of time shaving my legs, experimenting with the right position. This definitely included some failed experiments (I do not recommend the “swivel”-style device) … that resulted in hours of considerably painful tugging.
Very little sleep: extended catheter use can often result in bladder spasms; I was prescribed oxybutynin to deal with these. The most common side effect of oxybutynin is dry mouth, and it’s a humdinger, in my experience — I had an overwhelming urge to continuously drink water. This made sleep well-nigh impossible. There are tips online for dealing with the dry mouth, but these are all daytime stuff (chew gum, suck on ice) — you can’t do them while you’re sleeping. So I didn’t sleep much.
Given all the above, I am thrilled that the damn catheter is out of me, and I do hope the current adjustment period back to normal bladder function doesn’t last too long. I think my situation (catheter + ostomy) must be a fairly rare thing with LAR surgery patients; otherwise I think I would have had more instructions on how to get through it.